Our first ever worry about a pipe blockage feels like a very very long time ago. It was so stressful, not knowing why her bowel wasn’t releasing anything and wondering where it was going as a result. We are somewhat more used to it now, but that doesn’t make it any less worrying.
Blockages are now a daily occurrence. They can be minor, solved with a pipe squeeze, or, major, requiring a surgeon or doctor to aspirate her bowel and extract the contents with a large syringe.
The problem is the jejunostemy pipe. There’s a tiny pipe in her bowel – 1 of the 5 hours Clara was down for surgery was spent trying to find precisely the right size pipe. Too big or too small would mean the acid would leak inside her, and we certainly couldn’t risk that. This internal pipe connects to another, wider, pipe that sits externally. It’s in this external pipe we can see what fluid is (or isn’t as the case often is) coming out.
Blockages can occur in either pipe. Blockages in the external pipe are easy to see, but it’s impossible to know what’s going on internally.
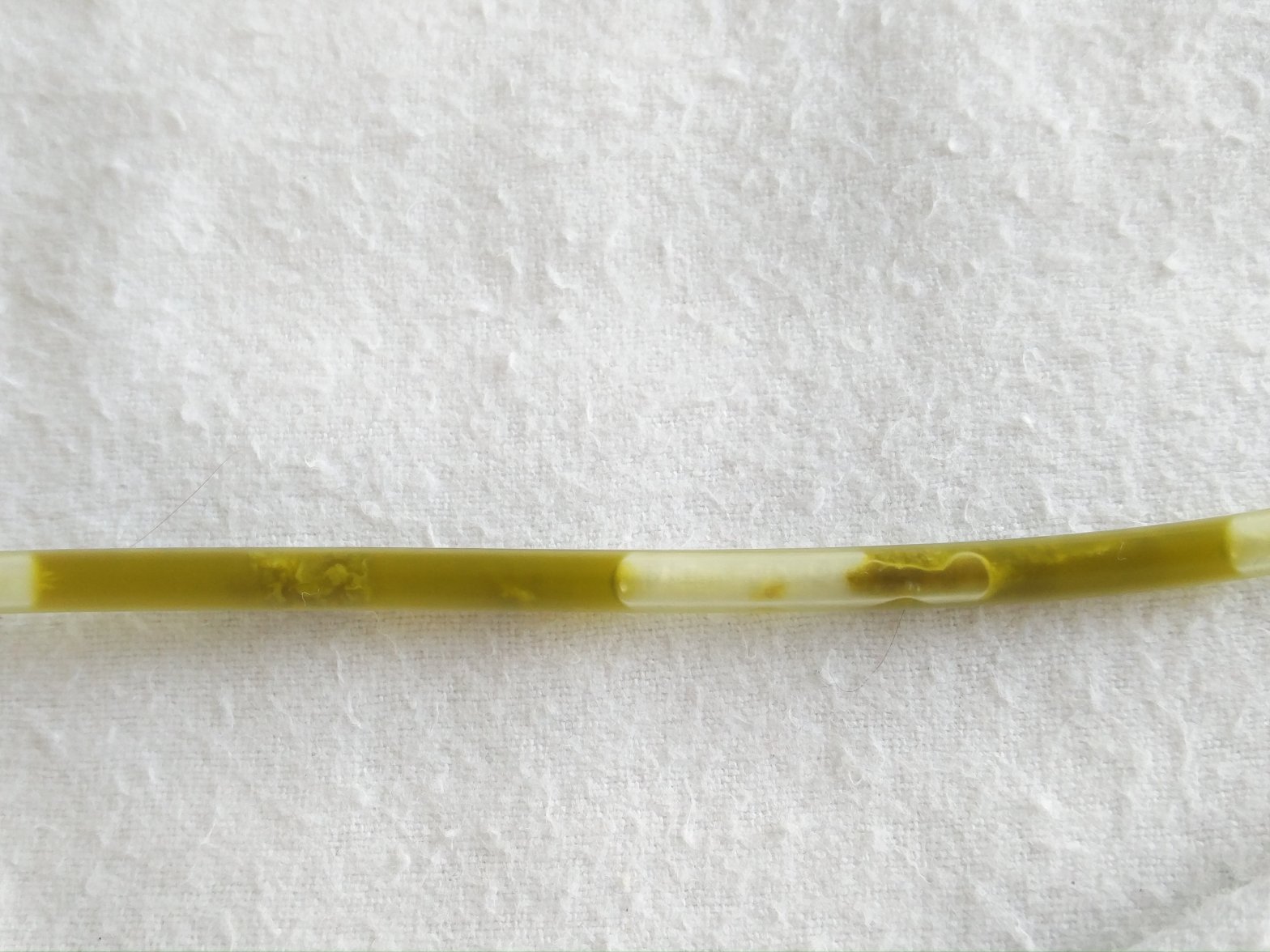
All of the green liquid shown in the picture below is stomach acid coming out of Clara via her external pipe. The darker green bits are what can block the pipe, both internally and externally. As you can see, she has quite a lot! If they get stuck in the wider external pipe, no wonder they get stuck in the tiny pipe inside her.

The jejunostemy pipe was the alternative to a stoma. Clara had too little bowel left to risk forming another stoma in her second operation. The first stoma she had was made up of bowel that then died off between her two operations. Creating another stoma required using more centimetres of bowel that she just didn’t have spare. The jejunostemy pipe has its risks though – regular blockages.
Interestingly, another surgeon said he would have created a stoma rather than the rare jejunostemy pipe. It just shows the importance of sticking with one surgeon continuously – Mr Lee knows Clara inside and out.
Right now Clara is very unsettled and won’t lie in her cot without crying and kicking her legs around. Even picking her up at times doesn’t settle her. Leaving her to cry is an option, but it’s hard on an open ward with other parents and babies trying to rest and recover. It doesn’t seem fair.
It could be that she didn’t sleep well last night (she finally fell asleep at 7am this morning) and so she’s just tired. It could be that her tummy is empty as she’s had regular waste output today. It could be that her tummy is still full somehow, she’s had a lot out but still less than recently. It could be she’s just being a baby!
The surgical registrar has been called to come and see her just in case. We need to make sure the internal pipe is actually still in her bowel.
I don’t have a gut feeling this time (‘scuse the pun) – I just know she’s not herself.

We are so with you at this time and just wish there was something we could do . Lots of love to the Family Smithson
LikeLike